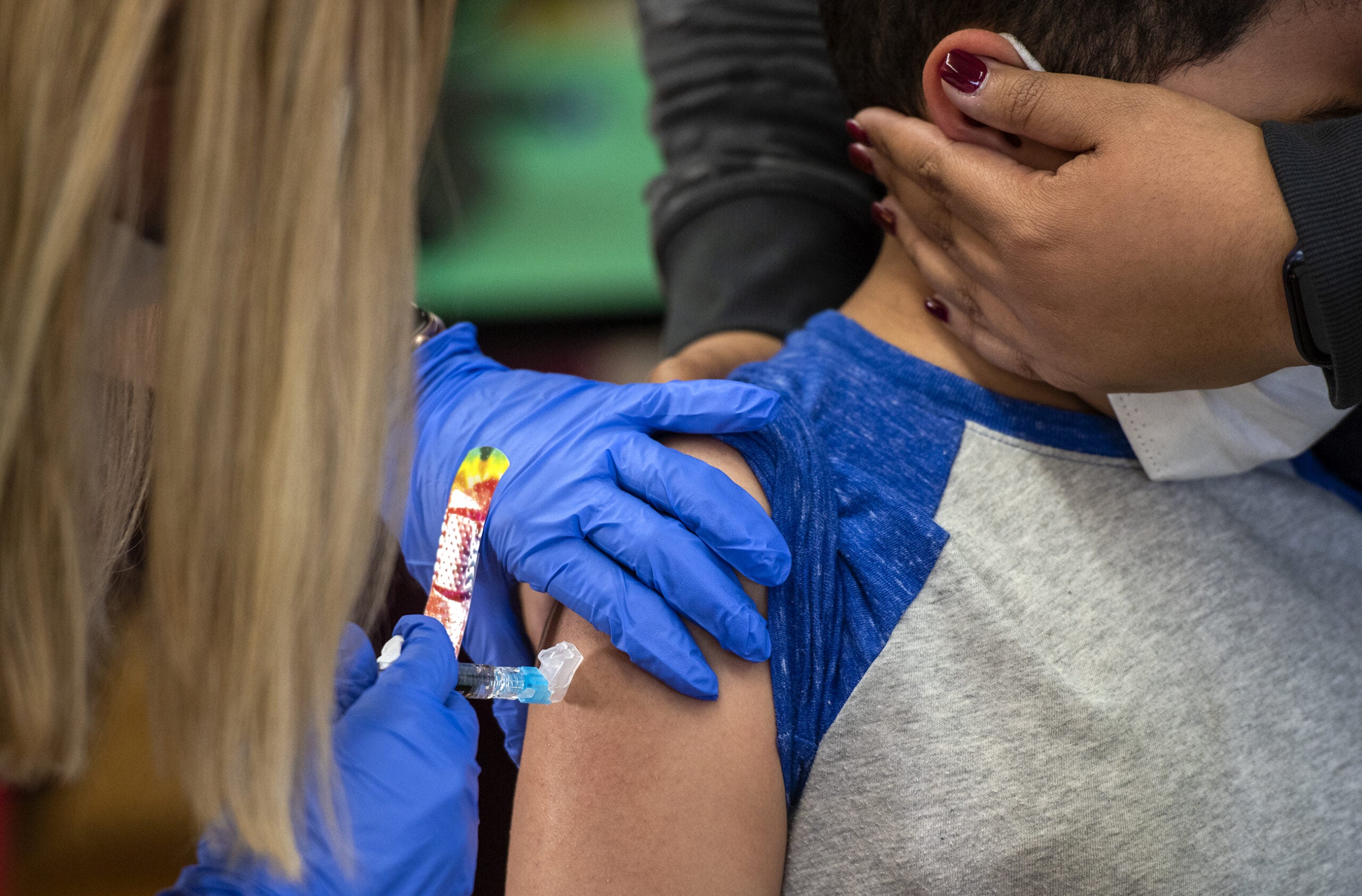


Alarmed by “near-exponential” growth in COVID-19 cases across Wisconsin, Gov. Tony Evers on Sept. 22 declared his third public health emergency during the pandemic and extended a statewide mask mandate to Nov. 21. The governor blamed a September spike in cases on young people eschewing distancing practices as universities started a new semester with in-person classes.
Evers pointed to state data to make the case that a mask mandate remained an essential tool for fighting the virus.
News with a little more humanity
WPR’s “Wisconsin Today” newsletter keeps you connected to the state you love without feeling overwhelmed. No paywall. No agenda. No corporate filter.
“New cases of COVID-19 slowed down in August as a result of the [mask] mandate, but as campuses reopened the last several weeks, there has been a new surge in cases across our state,” his office said in a press release.
Opposing the Democratic governor’s action, Republican lawmakers cited COVID-19 data to reach another conclusion.
“Data is in: masks either hurt or do not seem to make a difference,” said Rep. Scott Allen, R-Waukesha, in a press release flagging “the large growth in COVID-19 positive tests since this mandate was put into place in late July.”
The scientific evidence is clear: Widespread and proper use of face masks limits transmission of the coronavirus, as do physical distancing and handwashing. But contradictory messages from state leaders illustrate how data alone cannot help Wisconsinites agree on how to respond to a politicized pandemic that has infected at least 125,161 residents and killed 1,348 as of Oct. 1.
Wisconsin’s public health agencies each day release a deluge of data about where and how quickly COVID-19 is spreading. The river of information helps communities gauge everything from where to expect new outbreaks to which hospitals are likely to see a flood of patients. And the data have helped businesses, school districts, media outlets and others evaluate the effectiveness of tools such as face masks, which have become a cultural and political flashpoint.
But the data are hardly perfect, particularly as underfunded public health agencies scramble to report them in real time. And as the wealth of information swells Wisconsin’s ranks of armchair epidemiologists, real and perceived gaps have fueled arguments from skeptics of public health actions and muddled the public’s understanding of the pandemic.
Unprecedented levels of data
The Wisconsin Department of Health Services, like other state health agencies, publishes nearly real-time data about topics ranging from COVID-19 cases, hospitalizations, deaths, testing capacity, outbreak investigations and demographic trends related to the disease.
Many local health departments offer additional data.
The La Crosse County Health Department tracks how quickly contact tracers alert people about potential exposures. It has also named establishments linked to outbreaks, but paused that practice. That was due to a surge in cases that made La Crosse one of the nation’s top virus hot spots in September and strained the agency’s capacity. The Washington Ozaukee Public Health Department names schools within its two-county jurisdiction where students or teachers have tested positive.
Choosing and calculating those metrics has proved challenging, public health officials say. That is partly due to the federal government’s lack of standardized reporting guidance and Wisconsin’s sprawling public health apparatus. An example of this dynamic: daily differences between the data local health authorities and the state Department of Health Services report.
Dr. Ryan Westergaard, state epidemiologist for communicable diseases, defended Wisconsin’s COVID-19 data practices during a July 30 media briefing. Citing the uniquely urgent circumstances of the pandemic, Westergaard said discrepancies are bound to occur when so many agencies are releasing data every day.
“The standard that we as a state health department and a lot of our county and local partners have of sharing data at this level, meaning individual case counts on a daily basis, is truly without precedent at any level of public health,” said Westergaard, noting that agencies typically release similar data for other diseases monthly or annually to allow time for analysis and to correct errors.
“Because this is of such historical interest and [is] such a pressing public health crisis that everyone wants to know as much as possible [about], we’ve adopted this standard of sharing data on a daily basis,” he added.

The Department of Health Services’ “Outbreaks in Wisconsin” listing offers the state’s most comprehensive source of COVID-19 data. Before the pandemic, this inventory provided basic information about recent outbreaks of foodborne illness and rare infectious diseases. It has since transformed into an assortment of spreadsheets, graphs and maps depicting COVID-19’s impact on Wisconsin.
But the state’s data visualizations can confuse the casual observer and require close examination. Some visualizations define various metrics, such as new case counts and testing totals, differently depending on the context.
The free-flowing data has inundated health agencies with questions from news media and other members of the public since March, and short-staffed communications offices have struggled to keep up. And for the interest of time, the state health department limits news organizations to just one question during the agency’s semi-regular media briefings.
These gatekeeping practices have at times allowed data confusion to fester.
For instance, questions from WisContext about how the state defines and tracks COVID-19 cases labeled “active” and “recovered” extended for weeks as reporters exchanged sometimes confusing messages with state health department staffers about the meaning of these terms and availability of data. As it turns out, the definition for “recovered” cases is ripe for misinterpretation; it simply means patients are no longer considered infectious — not necessarily that they have overcome symptoms.
Still, the state agency occasionally makes data experts available to sort out confusion. It also published a series of explanations about how to interpret its data.
“We’ve had a lot of conversations recently about this,” said Traci DeSalvo, acting director for the state’s Bureau of Communicable Diseases, adding that the agency has no room to hold back more complex data — even at the risk of public misinterpretation. “It’s really a transparency thing and wanting to be consistent with what other states are doing,” DeSalvo said.
Data bottlenecks fuel suspicions
Wisconsin’s COVID-19 data primarily flows through the Wisconsin Electronic Disease Surveillance System, a secure database where healthcare providers and laboratory technicians upload reports about test results. The system provides a central clearinghouse for case and testing information related to a number of reportable diseases, including influenza, HIV/AIDS and now COVID-19.
Some local health officers have criticized the surveillance system as ill-equipped to handle the urgent needs of their departments as the disease surges across Wisconsin.
They include Jeanette Kowalik, the former health commissioner for the city of Milwaukee, who in late September joined the growing ranks of public health officials leaving their positions amid the pandemic’s tumult.
Kowalik, who took a job with a Washington, D.C.-based health policy organization, called Wisconsin’s surveillance system “an archaic technology” that wasn’t built to handle the steady waves of daily test data.

Among Kowalik’s frustrations with the system: Local health departments can’t automatically tally negative COVID-19 test results from within their communities. Instead, workers must first manually confirm each negative result.
“For that not to be automated has created a huge bottleneck for us,” Kowalik said.
This limitation has led to reporting bottlenecks in multiple communities. A Dane County backlog of negative results temporarily inflated the county’s rate of positive tests — a crucial statistic for measuring outbreaks.
The episode led some critics, including Republican leaders in the state, to accuse officials in Dane County, a Democratic stronghold, of intentionally inflating positivity rates to justify its pandemic public health restrictions, which are among the most stringent in the state.
“While processing negative tests is cumbersome there is no reason the counties intent on living shut down cannot keep up,” Washington County Executive Josh Schoemann tweeted on July 24 in response to a Milwaukee Journal Sentinel article about Dane County’s reporting backlog. “In [Washington County], we have the team in place to contract [sic] trace positives & notify negatives. Living w/ COVID takes leadership, not lockdowns.”
Kirsten Johnson, health officer for Washington and Ozaukee counties, said that problems with manually entering negative test results in the surveillance system prompted her team to refrain from reporting positivity rates during much of the pandemic.
“It’s just the way the system is set up, and it’s been a huge challenge for everyone since March,” Johnson said. “It’s time consuming, and it takes a lot of human capital to do it.”
Staff are in short supply at chronically underfunded public health departments that have barely coped with the herculean task of responding to COVID-19. Budget boosts during the pandemic have largely funded testing and contact tracing efforts.

Just one full-time Washington Ozaukee Health Department employee manages the flow of COVID-19 data from the surveillance system, spending most time tallying negative results, Johnson said.
Johnson looks forward to a long-promised system update that would allow local health departments to automatically tally negative results.
Department of Health Services Secretary-designee Andrea Palm said in a Sept. 24 media briefing that an upgrade to the system remained in the early planning stages. The changes will also streamline contact tracing, another area in which local health departments have struggled to keep up, Palm said.
Transparency and trust
Wisconsinites can gaze across the Mississippi River for a prominent example of the high stakes of processing and publishing COVID-19 data.
The Iowa Department of Public Health lost public trust after acknowledging in August a glitch in its COVID-19 data reporting system. The flaw erroneously lowered the state’s case numbers, and it fueled concerns about how the state calculated a key metric for assessing the safety of returning to in-person K-12 schooling.
Iowa Gov. Kim Reynolds, a Republican, made returning to in-person instruction a top priority, and barred districts from moving any instruction online unless 15% or more of local tests return positive over a two-week period.
However, the Iowa health department’s 14-day test-positivity statistics do not align with those local media have calculated based on the state’s own public data, and officials haven’t clearly explained the discrepancies.
Sowing more confusion, a state health department spokesperson in August erroneously said Iowa was calculating the 14-day metric by averaging daily positivity rates over the two-week period — instead of dividing all confirmed cases by all test results. Wisconsin officials say the described method skews the data, overweighting results on days with lower numbers of tests reported. In fact, Iowa’s COVID-19 dashboard indicates the state calculates the metric in the same way as Wisconsin, despite the spokesperson’s statements to the contrary.
The errors and inconsistencies eroded trust between Iowa’s state and local health officials during the crucial lead up to the new school year. Leaders of Iowa’s largest school district in Des Moines even defied the state’s demands to hold in-person instruction at the beginning of the school year, openly questioning the integrity of its metrics and public health advice.

Health officials across Wisconsin say they continue to err on the side of data transparency — even at the risk of sparking confusion or suspicions with imperfections.
To that end, on Sept. 30, the Wisconsin Department of Health Services unveiled new COVID-19 data metrics on its website. Among the updates were charts comparing two of the most common methods for calculating test-positivity rates: by tests and by people.
Previously, the state published data based solely on positivity among individuals newly tested, along with those who tested positive after previously testing negative. But as more people receive repeat negative test results, the state’s calculations have increasingly diverged from those calculated by the U.S. Centers for Disease Control and Prevention, which are based on total tests. The state’s new visualizations allow a quick comparison of the two methodologies.
Kirsten Johnson, the Washington and Ozaukee County official, said her joint health department draws on what she learned from researching the 1918 influenza pandemic, when Wisconsin’s robust public health system limited statewide deaths from a disease that killed an estimated 675,000 people across the nation.
“The communities that fared the best were the ones who were most transparent with the information they had,” Johnson said. “So that was sort of our guiding value going into this, and that’s still our value.”
This article was produced in collaboration with Wisconsin Watch.

This report was produced in a partnership between Wisconsin Public Radio, PBS Wisconsin and the University of Wisconsin Cooperative Extension. @ Copyright 2026, Board of Regents of the University of Wisconsin System and Wisconsin Educational Communications Board.